Bladder Cancer Insights
Why testing for FGFR genetic alterations is crucial
Bladder cancer is one of the most prevalent cancers of the urinary tract. It is also one of the most expensive cancers for healthcare systems due to its high recurrence rate.
Molecular stratification of bladder cancer has become more important as targeted therapy options expand. A range of immunotherapies and targeted therapies are already approved for eligible patients, with more being in clinical evaluation.
Bladder Cancer Overview

Epidemiology of bladder cancer
Since 2020, global incidence of bladder cancer has increased by 7.1%, ranking it the 9th most frequently diagnosed cancer worldwide.
Men over the age of 55 are most affected. In Europe, bladder cancer is the 4th most common cancer in men.
Disease characteristics
90% of bladder cancers originate in the urothelium (urothelial carcinoma).
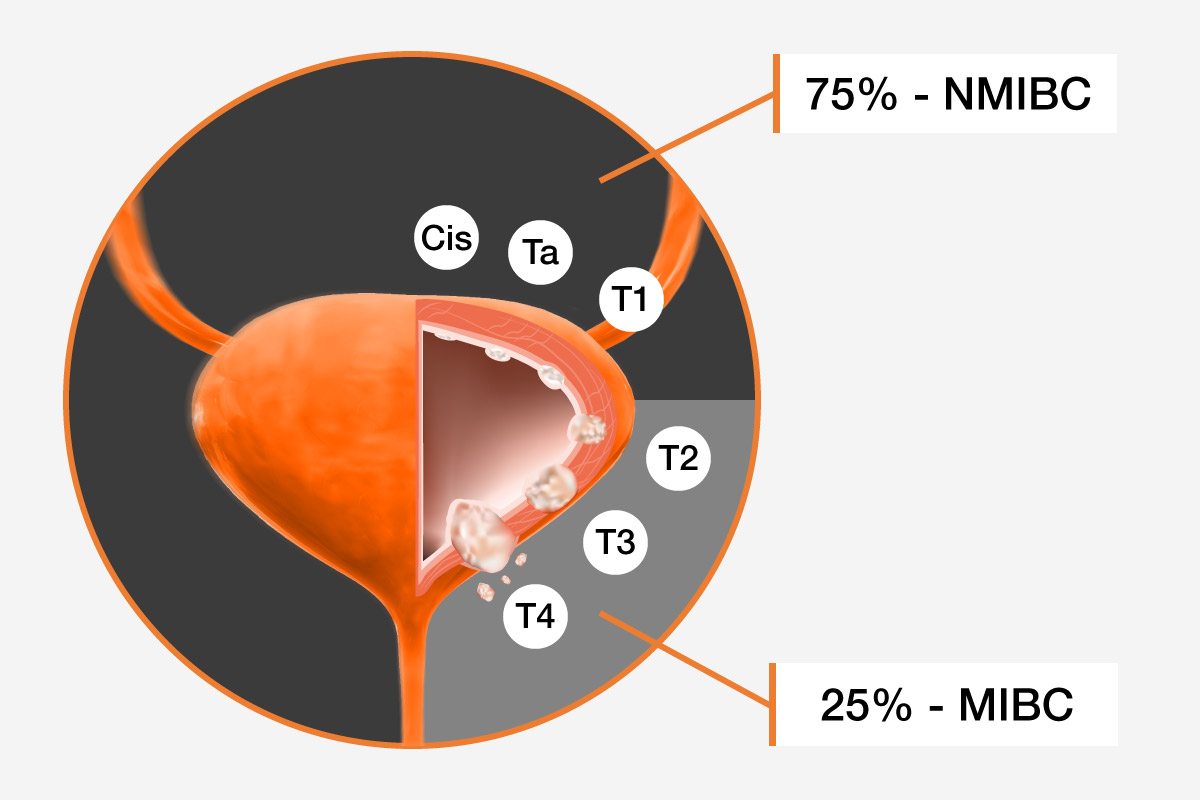
Non-muscle invasive bladder cancer (NMIBC):
- Includes Cis, Ta and T1 stages
- Tumor has not penetrated the muscle layer
- High recurrence rate
- Includes Cis, Ta and T1 stages
- Tumor has not penetrated the muscle layer
- High recurrence rate
Muscle invasive bladder cancer (MIBC):
- Includes T2-T4 stages
- Tumor has spread into or through the muscle layer
- Includes T2-T4 stages
- Tumor has spread into or through the muscle layer
Metastatic bladder cancer (T4) is associated with a poor prognosis.
Role of FGFRs as Biomarkers in Bladder Cancer

Molecular profiling of bladder cancer
Malignant tumors harbor multiple genetic alterations driving tumor development. These alterations can give valuable insights into prognosis and response to therapy when examined by researchers, pathologists, and clinicians.
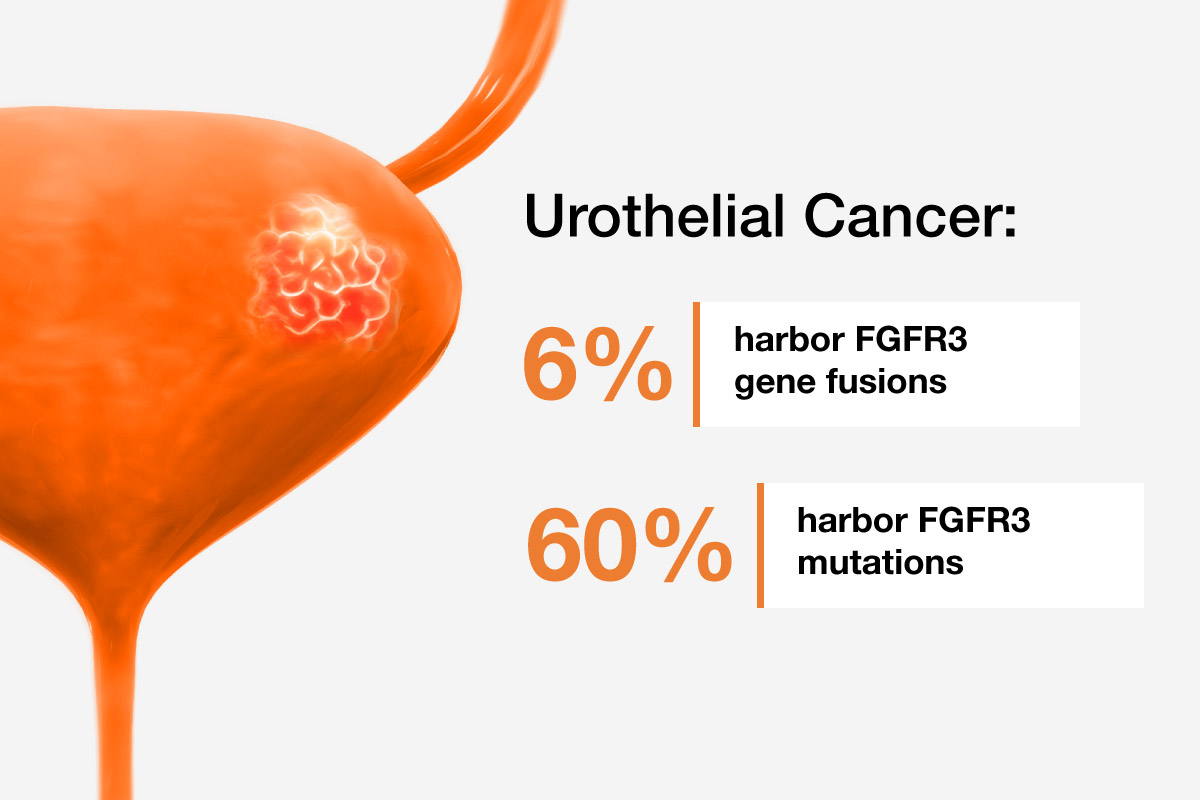
Fibroblast Growth Factor Receptor 3 (FGFR3) as a biomarker
FGFR3 is one of the most affected genes in bladder cancer, including both missense mutations and gene fusions. Consequently, FGFR3 has become the focus for selective inhibitor development.
Products for FGFR Testing


Therapeutic Options for Bladder Cancer
Initial management of bladder cancer may involve:
- Surgical removal of the tumors
- Bacillus Calmette-Guérin (BCG) treatment, intravesical immunotherapy using Mycobacterium bovis Bacillus Calmette-Guérin
- High-risk or BCG-unresponsive NMIBC and MIBC can require complete bladder removal (radical cystectomy)
- Surgical removal of the tumors
- Bacillus Calmette-Guérin (BCG) treatment, intravesical immunotherapy using Mycobacterium bovis Bacillus Calmette-Guérin
- High-risk or BCG-unresponsive NMIBC and MIBC can require complete bladder removal (radical cystectomy)
Treatment of advanced bladder cancer can include various drug regiments:
Chemotherapy
Platinum-based chemotherapy
- For example, Gemcitabine-cisplatin, Gemcitabine-carboplatin
- Crosslink DNA, block cell replication, cause cell death
Immunotherapy
Immune Checkpoint Inhibitors
- For example, Pembrolizumab, Avelumab, Nivolumab
- Block PD-L1+PD-1 interaction, preventing immune evasion
ADCs
Antibody-drug conjugates
- Example, Enfortumab vedotin
- Targets NECTIN-4 on the tumor cell surface, which is often overexpressed in urothelial cancer
- Binding triggers internalization and delivers a microtubule inhibitor to these cells causing tumor cell death
FGFR Inhibition
Erdafitinib
- A small molecule inhibitor targeting FGFR1-4
- Recommended for pre-treated urothelial tumors harboring driver FGFR2/3 fusions and FGFR3 missense mutations
Identifying biomarkers such as FGFR3 may enable a wide range of personalized therapy decisions.
Clinical Trials Finder
Find clinical trials in bladder cancer near you: